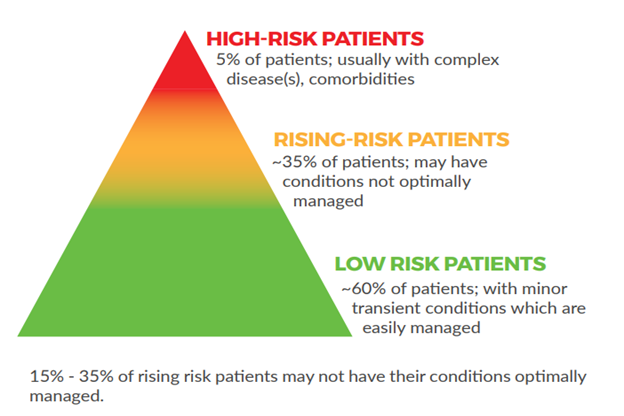
Care planning will provide the greatest value when patients who can benefit most from care planning are targeted. From the literature, the suggested target population are those patients who have complex health needs with conditions that are not optimally managed (also known as ‘rising risk’). However, it can be a challenge to identify who these patients are.
Care planning should be proactive and anticipatory. Teams need a way to routinely identify eligible patients, offer care, and book longer appointments.
Approaches to Identifying Patients
There are a number of ways that teams can identify patients who may benefit from a care plan. Some examples include:
Start with those who qualify for a Comprehensive Annual Care Plan (billing code: 03.04J) and then determining who on that list has the greatest need
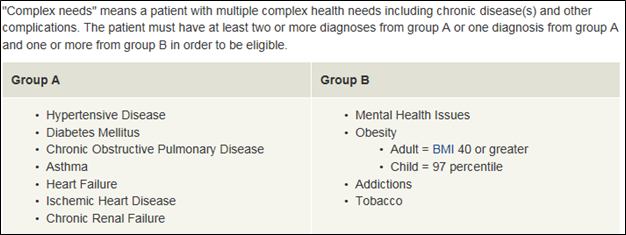
Figure 1. For claiming the 03.04J billing code, a patient must have at least 1 condition from Group A and 1 condition from Group B, or two conditions from Group A.
Consider the two patients below. While both qualify equally for a care plan, there is potential for Patient B to receive greater benefit.
| Patient A | Patient B |
|
|
Use the HQCA Primary Healthcare Panel Report to determine who falls within the Clinic Risk Group number 5-7
Clinic Risk Grouper (CRG) levels were developed as a tool to assess and classify individual patients according to the severity of chronic and acute illness and projected costs to the healthcare system. The CRG levels are classified as follows:
Level 1 (Healthy) Level 2 (History of significant acute disease)
Level 3 (Single minor chronic disease)
Level 4 (Minor chronic disease in multiple organ systems)
Level 5 (Single dominant or moderate chronic disease)
Level 6 (Significant chronic disease in multiple organ systems)
Level 7 (Dominant chronic disease in three or more organ systems)
Level 8 (Dominant, metastatic, and complicated malignancies)
Level 9 (Catastrophic conditions)
As continuity for all patients increase, cost of care decreases. This also holds true for the highest cost groups.
Use a combination of clinical criteria, risk factors and utilization parameters
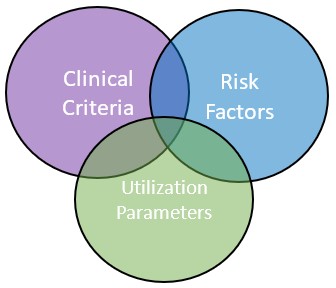 Table 1. Menu of clinical criterial, risk factors and utilization parameters to consider when identifying your population for care planning.
Table 1. Menu of clinical criterial, risk factors and utilization parameters to consider when identifying your population for care planning.
| Clinical Criteria | Risk Factors | Utilization Parameters |
|
|
|
Using the EMR
1. Use EMR to generate a list
- Start to identify patients “not managed”
- Run a list of patients not seen in a year over the age of (75 or 80 or 85)
- Consider menu of criteria in Table 1
2. Review the list as a team
- Add columns to the list of patients for more information
- Seek additional information in the chart, as needed
3. Select first cohort of patients
- Start with the ‘low hanging fruit’
- Use the list to reach out to patients to offer care planning
4. Create processes in the EMR to identify the patient as part of a specific population for care planning
- Add to the Problem List or Profile/Medical History Band
- “Complex Health Needs”
- Be consistent
- Agree on protocol
- This is essential for monitoring and measurement
Developed by
