The Patient’s Medical Home is the practice patients feel most comfortable attending for their primary care needs. The optimized Patient’s Medical Home (PMH) emphasizes the role of an interdisciplinary team that provides high-quality, comprehensive, compassionate and timely care.
Optimizing Patient’s Medical Home can lead to:
- increased patient and provider satisfaction
- improved quality of care
- reduced costs
- reduced hospitalizations
Source: Evidence summary: Benefits of the PMH
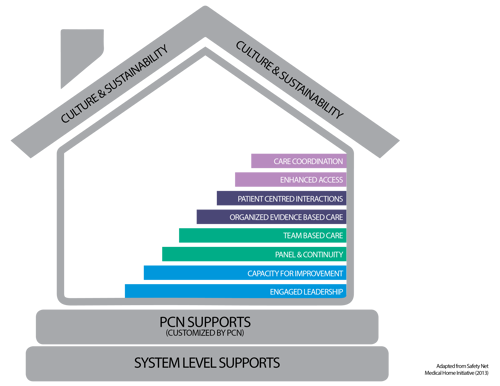
How to Optimize the Patient’s Medical Home?
Optimizing the PMH can be achieved by focusing on 8 key implementation elements.
Learn more about each and resources available to support your clinic or Primary Care Network (PCN):
Leaders in medical homes work with the clinic team to remove barriers and support continuous forward momentum towards PMH goals. Physician leaders are encouraged to partner with Practice Facilitators to support PMH improvement with teams and promote the PMH with their PCN and physician peers.
Key Resources:
Physician Leadership Network PMH Podcast Physician Champions Literature SummaryHaving a quality improvement (QI) strategy in place to help give clinic teams confidence, skills and a specific organized approach to making changes with the roles like Practice Facilitators and Physician Champions defined to support change and quality improvement work.
Key Resources:
Practice Facilitation Resources Practice Facilitation Training Networks of Practice Quality Improvement Resources
In the most basic definition, panel is the group of patients who consider a physician to be their primary care provider, and that physician agrees. Providers ensure they confirm their patient panels on a regular basis and use the panel list to proactively manage their health needs.
Continuity of care reflects the patient’s experience of care over time as consistent, connected and coordinated.
Key Resources:
Panel Processes Change Package Summary Relational Continuity Change Package Summary Evidence Summary: The Benefits of Relational Continuity Panel in Action Training STEP Toolkit Relational Continuity CII/CPAR Resources
In an optimized PMH, care is provided by an interdisciplinary team working at their full scope of practice, led by the physician, and includes a variety of skill sets designed to meet the needs of the panel.
Key Resources:
Team Based Care Roles and Responsibilities Template Introductions with Intention Team Huddles GuideIn an optimized PMH, evidence-based guidelines are embedded into daily clinical practice and shared with patients. Each encounter is designed to meet the patient’s acute, preventive and chronic illness needs, using planned interactions and ensuring appropriate follow-up care.
Key Resources:
Alberta Screening and Prevention (ASaP) Alberta Screening and Prevention Plus (ASaP+) Clinical Practice Guidelines Primary Health Care Opioid ResponseIn an optimized PMH, patients’ values and preferences are respected, and they (and family members) are encouraged to be actively involved in making decisions about their health. Communication with patients is prioritized and involves language they understand. Patients are regularly asked for feedback on how the clinic team can make the experience at the clinic better.
Key Resource:
Care Plan Template with PromptProviding timely access to one’s primary care physician is a key implementation element of an optimized Patient's Medical Home. This can be achieved by balancing supply and demand.
Key Resources:
Enhanced Access ResourcesThe goal of care coordination is to make the family practice the centre of care for the patient. Care must be coordinated not only within the medical home, but also between the:
- medical home
- health neighbourhood
- broader healthcare system
When referrals are made, communication occurs between providers so the patient doesn’t have sole responsibility to remember details of their history, diagnosis or care plan.
Key Resources:
Home to Hospital to Home (H2H2H) Transitions Reducing the Impacts of Financial StrainFoundational enablers
Foundational to an optimized Patient’s Medical Home are clinic enablers, Primary Care Network enablers and system-level supports. To learn more about each enabler, and what resources there are to support them, please see key resources below.
Electronic Medical Record Supports Physician CompensationPatient's Medical Home Assessment Tool
Want to assess your clinic’s progress in optimizing the Patient’s Medical Home? Consider using the PMH Assessment tool.
PMH Assessments