Case
Kanwar, a 72-year-old male with acute decompensated heart failure, was initiated on Lasix. Though his symptoms improved, his energy levels remained suboptimal. An echocardiogram was requested and the workup for contributing factors was unremarkable.
Part 2: Objectives
- Investigate guideline-directed medical therapy (GDMT).
- Personalize GDMT based on comorbidity profile.
- Tailor treatment considering "intrinsic capacity" or "biologic age."
- a. Employ non-pharmacological management strategies.
- b. Utilize pharmacological strategies.
Background
Heart failure is frequently underdiagnosed, particularly in frail individuals with atypical presentations. Only 13.2% of heart failure patients aged ≥65 years receive optimal Guideline-Directed Medical Therapy (GDMT).1-8
Chronological age presents a heterogeneous and limited parameter for individual diagnosis, prognosis and treatment recommendations, extending beyond heart failure to various clinical scenarios. Multiple tools are accessible for evaluating "biological age," "intrinsic capacity" or "physiological reserves," such as the clinical frailty scale.9-15
Evidence
Precipitating factors
Exploring potential precipitating factors for heart failure is essential, including non-adherence to diet or medication, anemia, arrhythmia, infection, inflammation and more.16
Pharmacological therapy
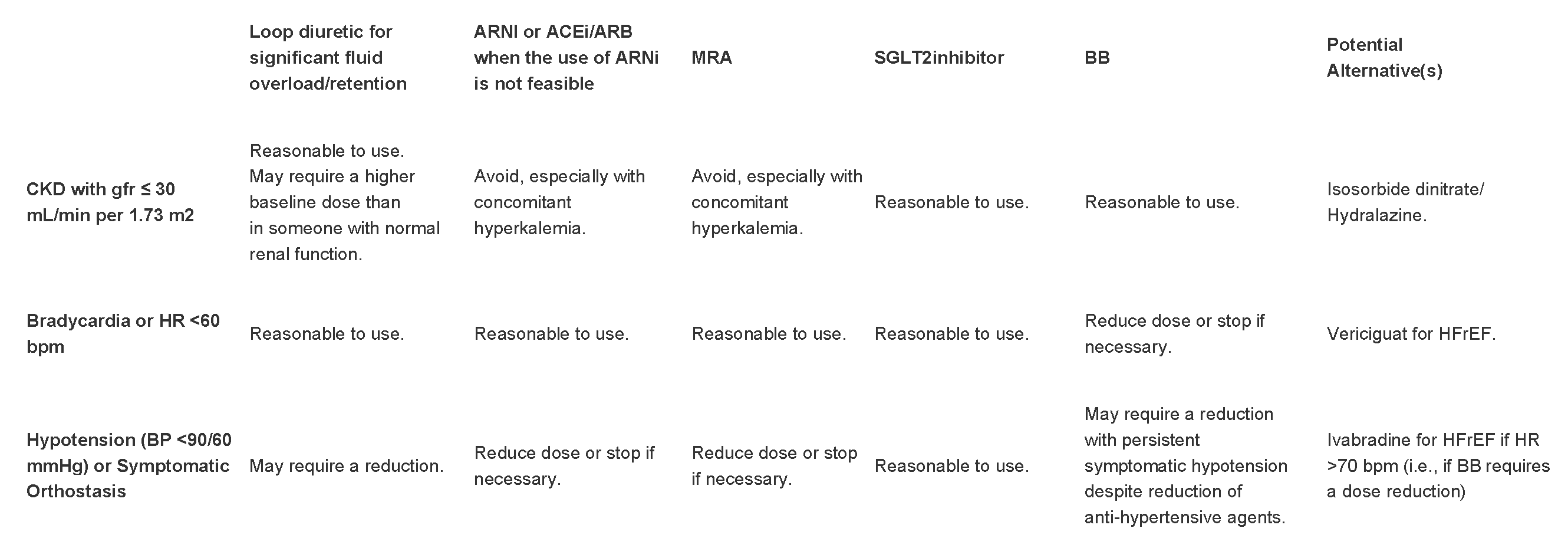
Pharmacological therapy involves standard GDMT: ACE inhibitors (ACEi) or angiotensin receptor blockers (ARB), beta-blockers (BB), mineralocorticoid receptor antagonists (MRAs) and SGLT2 inhibitors. Loop diuretics are indicated in patients with functionally limiting edema. Other pharmacological treatments for heart failure include Digoxin, Isosorbide dinitrate/hydralazine, Ivabradine and Vericiguat. Their evidence for benefit is not as strong as GDMT.17-21 GLP-1 agonists have shown mixed results in heart failure patients.22,23
Definitions
GDMT is based on LVEF and NYHA classification.17-19, 21
Two strategies for sequencing GDMT exist: conventional and proposed new.
The conventional sequence: ACEi or ARB → beta-blocker → MRA → ACEi or ARB switch to ARNI (ideal but not common) → SGLT2i over 24 weeks. Up titration to target doses at each step.
The proposed new sequence: beta-blocker + SGLT2i → ARNI → MRA over four weeks. Up titration to target doses thereafter.18
Table 1: Heart failure types based on LVEF
|
Heart failure (HF) with a reduced ejection fraction (HFrEF) |
LVEF ≤ 40% |
|
Heart failure (HF) with a reduced ejection fraction (HFrEF) HF with a mid-range ejection fraction (HFmEF) |
LVEF ≤ 40% LVEF 41-49% |
|
Heart failure (HF) with a reduced ejection fraction (HFrEF) HF with preserved ejection fraction (HFpEF) |
LVEF ≤ 40% LVEF ≥ 50% |
Table 2: New York Heart Association (NYHA) functional classification
|
Class I |
No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF. |
|
Class I Class II |
No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF. Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in symptoms of HF. |
|
Class I Class III |
No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF. Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes symptoms of HF. |
|
Class I Class IV |
No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF. Unable to perform any physical activity without symptoms of HF, or symptoms of HF at rest. |
Table 3: Treatment based on LVEF and NYHA
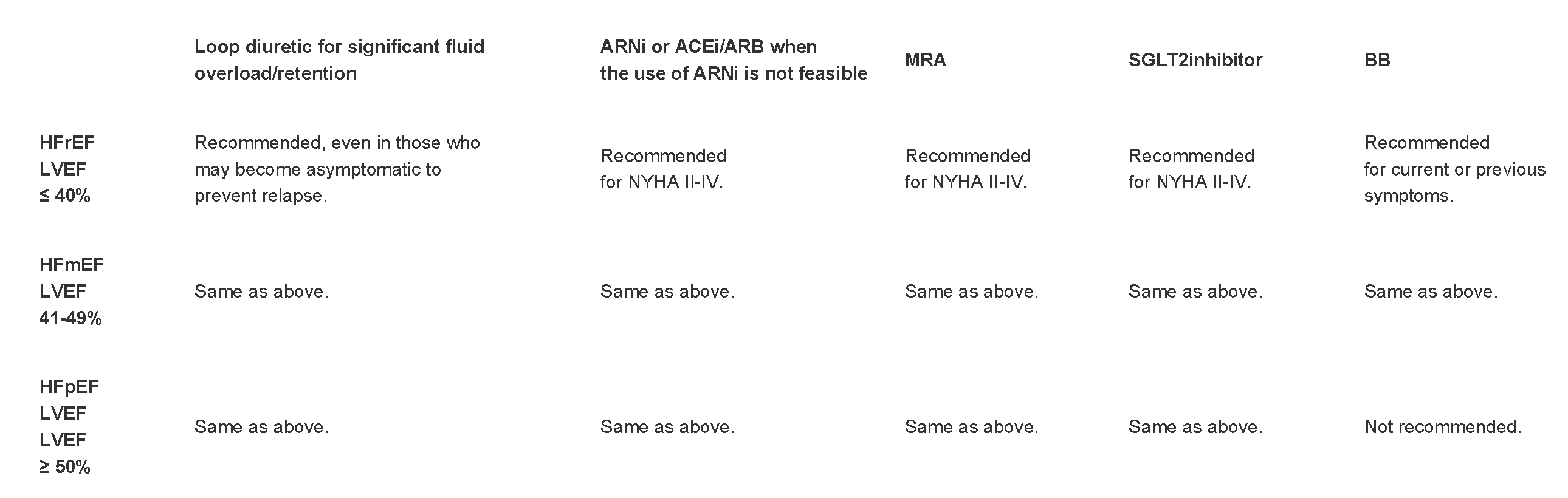
Table 4: Tailoring GDMT based on heart failure and comorbidity profile
Non-pharmacological therapy for patients with heart failure
This includes exercise, sodium intake limitation, CPAP for sleep apnea, vaccines, smoking cessation, weight management, alcohol reduction and primary disease prevention.19,21 Some HFrEF patients benefit from device therapies like ICDs and CRTs, typically once on optimal GDMT.19,21,25,26
Tailoring non-pharmacological and pharmacological therapy based on intrinsic capacity
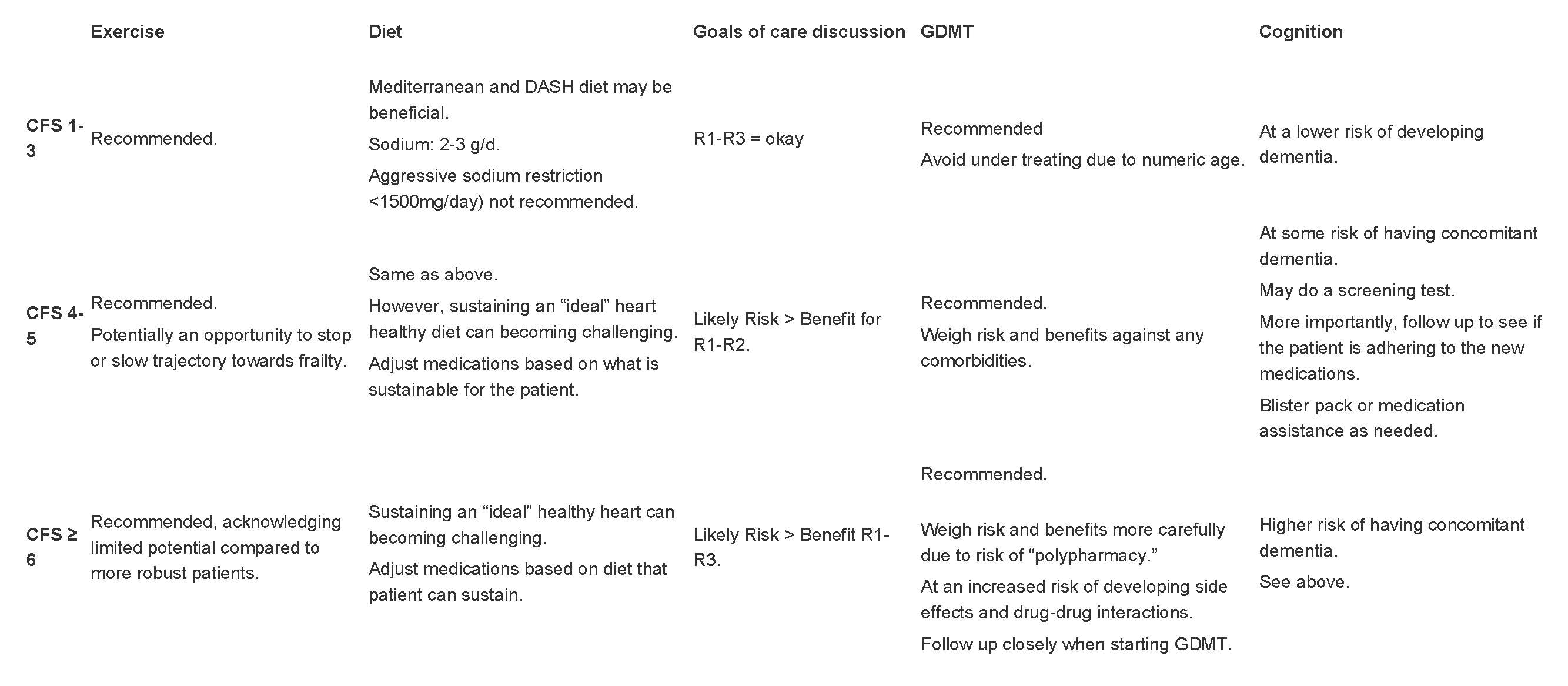
Though not common, emerging evidence supports stratifying patients based on their physiological reserves. Here are some recommendations based on evidence and expert advice:18,19,21,27-31,33,34,35
Table 5: Management Strategies based on extent of intrinsic capacity or physiological reserves
Back to the case
Echocardiogram: LVEF 35% with no significant valvulopathy.
Creatinine and electrolytes within normal limits on Lasix and ACEi.
Heart rate: 60-70 bpm on the beta-blocker.
Euvolemic status: Resolved symptoms at rest, NT-ProBNP = 300 pg/mL and improved chest X-ray.
Patient is mildly frail (CFS 5/9) reflected by a three-year decline and four-month deconditioning.
Pharmacological and non-pharmacological management strategies
GDMT: Started on low-dose Spironolactone 12.5mg. Send referral to the heart function clinic.
Exercise: Recommended at least three times a week, including balance, resistance and aerobic exercises. Suggesting a personal trainer due to the patient's unfamiliarity with exercises.
Diet: Suggested Mediterranean or DASH diet, supported by the patient's wife.
Cognition: No need for medication blister packing; the patient can manage his own medications and booking appointments.
Goals of care: Discussed and patient chose M1 goals of care based on baseline reserves.
Summary
Acute decompensated heart failure with volume overload: Optimize diuretic strategy.
Symptomatic heart failure: Echocardiogram. Optimize GDMT based on EF, NYHA, comorbidity profile and intrinsic capacity.
Non-pharmacological strategies, goals of care discussions and addressing adherence risk should align with the patient's intrinsic capacity or reserves.
Please see the CCS HF guidelines to help guide therapy in patients with heart failure.
References
- Long B, Koyfman A, Gottlieb M. Diagnosis of Acute Heart Failure in the Emergency Department: An Evidence-Based Review. J Am Geriatr Soc. 1989; 37: 423-9.
- Oudejans I, Mosterd A, Bloemen JA, Valk MJ, van Velzen E, Wielders JP, Zuithoff NP, Rutten FH, Hoes AW. Clinical evaluation of geriatric outpatients with suspected heart failure: value of symptoms, signs, and additional tests. J Am Geriatr Soc. 1989; 37: 423-9.
- Barents M, van der Horst I, Voors A, Hillege J, Muskiet F, de Jongste M. Prevalence and misdiagnosis of chronic heart failure in nursing home residents: the role of B-type natruiretic peptides. J Am Geriatr Soc. 1989; 37: 423-9.
- Davies M, Hobbs F, Davis R, Kenkre J, Roalfe AK, Hare R, Wosornu D, Lancashire RJ. Prevalence of left ventricular systolic dysfunction and heart failure in the Echocardiographic Heart of England Screening study: a population based study. J Am Geriatr Soc. 1989; 37: 423-9.
- Hancock HC, Close H, Mason JM, Murphy JJ, Fuat A, Singh R, Wood E, de Belder M, Brennan G, Hussain N, Kumar N, Wilson D, Hungin APS. J Am Geriatr Soc. 1989; 37: 423-9.
- Bozkurt B, Coats AJ, Tsutsui H, Abdelhamid M, Adamopoulos S, Albert N, Anker SD, Atherton J, Böhm M, Butler J, Drazner MH, Felker GM, Filippatos G, Fonarol GL, Gomez-Mesa JE, Heidenreich P, Imamura T, Januzzi J, Jankowska EA, Khazanie P, Kinugawa K, Lam CS P, Matsue Y, Metra M, Ohtani T, Piepoli MF, Ponikowski P, Rosano GMC, Sakata Y, SeferoviĆ P, Starling RC, Teerlink JR, Vardeny O, Yamamoto K, Yancy C, Zhang J, Zieroth S. J Am Geriatr Soc. 1989; 37: 423-9.
- Glenny, C, Heckman, G, McKelvie, R. Heart Failure in older persons: considerations for the primary care physician. J Am Geriatr Soc. 1989; 37: 423-9.
- Wahid M, Aghanya V, Sepehrvand N, Dover DC, Kaul P, Ezekowitz J. Use of Guideline-Directed Medical Therapy in Patients Aged ≥ 65 Years After the Diagnosis of Heart Failure: A Canadian Population-Based Study. J Am Geriatr Soc. 1989; 37: 423-9.
- Tamara Mann, "Should Age Matter? How 65 Came to Be Old and Old Came to Be Ill", Origins: Current Events in Historical Perspective. December, 2012.
- Rabheru K, Byles JE, Kalache A. How “old age” was withdrawn as a diagnosis from ICD-11. Volume 3, Issue 7, E457-E459, July 2022.
- Muscedere J. The need to implement frailty in the International Classification of Disease (ICD). J Frailty Aging. 2020; 9: 2-3.
- Kehler DS, Ferguson T, Stammers AN, Bohm C, Arora RC, Duhamel TA, Tangri N. Prevalence of frailty in Canadians 18–79 years old in the Canadian Health Measures Survey. BMC Geriatr. 2017;17:28.
- Hamada T, Kubo T, Kawai K, Nakaoka Y, Yabe T, Furuno T, Yamada E, Kitaoka H, YOSACOI study group. Clinical characteristics and frailty status in heart failure with preserved vs. reduced ejection fraction. ESC Heart Fail. 2022 Jun;9(3):1853–1863.
- Rajabali N, Rolfson D, Bagshaw SM. Assessment and Utility of Frailty Measures in Critical Illness, Cardiology, and Cardiac Surgery. Can J Cardiol. 2016 Sep;32(9):1157-65.
- Sze S, Pellicori P, Zhang J, Weston J, Clark AL. Identification of Frailty in Chronic Heart Failure. JACC: Heart Failure. April 2019;7(4):291-302.
- Verdu-Rotellar, J. M., Vaillant-Roussel, H., Abellana, R., Jevsek, L. G., Assenova, R., Lazich, D. K., Torszai, P., Glynn, L. G., Lingner, H., Demurtas, J., Borgstrom, B., Gibot-Boeuf, S., & Munoz, M. A. (2020). Precipitating factors of heart failure decompensation, short-term morbidity and mortality in patients attended in primary care. SCANDINAVIAN JOURNAL OF PRIMARY HEALTH CARE, 38(4), 473-480.
- McDonald, M., Virani, S., Chan, M., Ducharme, A., Ezekowitz, J. A., Giannetti, N., Heckman, G. A., Howlett, J. G., Koshman, S. L., Lepage, S., Mielniczuk, L., Moe, G. W., O'Meara, E., Swiggum, E., Toma, M., Zieroth, S., Anderson, K., Bray, S. A., Clarke, B., Cohen-Solal, A., D'Astous, M., Davis, M., De, S., Grant, A. D. M., Grzeslo, A., Heshka, J., Keen, S., Kouz, S., Lee, D., Masoudi, F. A., McKelvie, R., Parent, M. C., Poon, S., Rajda, M., Sharma, A., Siatecki, K., Storm, K., Sussex, B., Van Spall, H., & Yip, A. M. C. (2021). CCS/CHFS Heart Failure Guidelines Update: Defining a New Pharmacologic Standard of Care for Heart Failure With Reduced Ejection Fraction. Can J Cardiol, 2022, 37, 531-546.
- MacDonald, B. J., Virani, S. A., Zieroth, S., & Turgeon, R. (2023). Heart Failure Management in 2023: A Pharmacotherapy- and Lifestyle-Focused Comparison of Current International Guidelines. VOLUME 5, ISSUE 8, P629-640, August 2023.
- Ezekowitz, J. A. (Chair, Primary Panel), O'Meara, E. (Co-chair, Primary Panel), McDonald, M. A. (Primary Panel), Abrams, H. (Primary Panel), Chan, M. (Primary Panel), Ducharme, A. (Primary Panel), Giannetti, N. (Primary Panel), Grzeslo, A. (Primary Panel), Hamilton, P. G. (Primary Panel), Heckman, G. A. (Primary Panel), Howlett, J. G. (Primary Panel), Koshman, S. L. (Primary Panel), Lepage, S. (Primary Panel), McKelvie, R. S. (Primary Panel), Moe, G. W. (Primary Panel), Rajda, M. (Primary Panel), Swiggum, E. (Primary Panel), Virani, S. A. (Primary Panel), Zieroth, S. (Primary Panel), Al-Hesayen, A. (Secondary Panel), Cohen-Solal, A. (Secondary Panel), D'Astous, M. (Secondary Panel), De, S. (Secondary Panel), Estrella-Holder, E. (Secondary Panel), Fremes, S. (Secondary Panel), Green, L. (Secondary Panel), Haddad, H. (Secondary Panel), Harkness, K. (Secondary Panel), Hernandez, A. F. (Secondary Panel), Kouz, S. (Secondary Panel), LeBlanc, M-H. (Secondary Panel), Masoudi, F. A. (Secondary Panel), Ross, H. J. (Secondary Panel), Roussin, A. (Secondary Panel), Sussex, B. (Secondary Panel). "Comprehensive Update of the Canadian Cardiovascular Society guidelines for the management of heart failure." Can J Cardiol, 2017, 33, 1342-1343.
- Vaduganathan, M., Claggett, B. L., Jhund, P. S., Cunningham, J. W., Ferreira, J. P., Zannad, F., Packer, M., Fonarow, G. C., McMurray, J. J. V., & Solomon, S. D. (2020). Estimating lifetime benefits of comprehensive disease-modifying pharmacological therapies in patients with heart failure with reduced ejection fraction: a comparative analysis of three randomized controlled trials. Lancet, 2022, 399, 1391-1400
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay, S.M., Evers, L.R., Fang, J.C., Fedson, S.E., Fonarow, G.C., Hayek, S.S., Hernandez, A.F., Khazanie, P., Kittleson, M.M., Lee, C.S., Link, M.S., Milano, C.A., Nnacheta, L.C., Sandhu, A.T., Stevenson, L.W., Vardeny, O., Vest, A.R., Yancy, C.W. (2022). 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol, 2022, 79, e263-e421.
- Kosiborod MN, Abildstrøm SZ, Borlaug BA, Butler J, Rasmussen S, Davies M, Hovingh GK, Kitzman DW, Lindegaard ML, Møller DV, Shah SJ, Treppendahl MB, et al. (2023). Semaglutide in Patients with Heart Failure with Preserved Ejection Fraction and Obesity. N Engl J Med, 2023, 389, 1069-1084.
- Oser J, Packer M, & Ferreira JP. (2023). Increased Risk of Heart Failure Hospitalization With GLP-1 Receptor Agonists in Patients With Reduced Ejection Fraction: A Meta-Analysis of the EXSCEL and FIGHT Trials. Journal of Cardiac Failure, 29(7): 1107-110.
- Rosano GMC, Moura B, Metra M, Böhm M, Bauersachs J, Ben Gal T, Adamopoulos S, Abdelhamid M, Bistola V, Celutkien J, Chioncel O, Farmakis D, Ferrari R, Filippatos G, Hill L, Jankowska EA, Jaarsma T, Jhund P, Lainscak M, Lopatin Y, Lund L.H., Milicic D, Mullens W, Pinto F, Ponikowski P, Savarese G, Thum T, Volterrani M, Anker SD, Seferovic PM, & Coats AJS. (2021). Patient profiling in heart failure for tailoring medical therapy. A consensus document of the Heart Failure Association of the European Society of Cardiology. European Journal of Heart Failure, 23, 872-881.
- Moss AJ, Hall WJ, Cannom DS, Daubert JP, Higgins SL, Klein H, Levine JH, Saksena S, Waldo AL, Wilber D, Brown MW, & Heo M. (1996). Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter Automatic Defibrillator Implantation Trial Investigators. N Engl J Med, 1996, 335(26), 1933-1940.
- Cleland JGF, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, Tavazzi L, & Cardiac Resynchronization-Heart Failure (CARE-HF) Study Investigators. (2005). The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med, 2005, 352(15), 1539-1549.
- Ezekowitz JA, Colin-Ramirez E, Ross H, Escobedo J, MacDonald P, Troughton R, Saldarriaga C, Alemayehu W, McAlister FA, Arcand J, Atherton J, Doughty R, Gupta M, Howlett J, Jaffer S, Lavoie A, Lund M, Marwick T, McKelvie R, Moe G, Pandey AS, Porepa L, Rajda M, Rheault H, Singh J, Toma M, Virani S, & Zieroth S. (2022). Reduction of dietary sodium to less than 100 mmol in heart failure (SODIUM-HF): an international, open-label, randomized, controlled trial. Lancet, 2022, 399, 1391-1400.
- Ibitoye SE, Rawlinson S, Cavanagh A, Phillips V, Shipway DJH. (2021). Frailty status predicts futility of cardiopulmonary resuscitation in older adults. Age Ageing, 2021, 50(1), 147-152.
- Hu FY, Streiter S, O'Mara L, Sison SM, Theou O, Bernacki R, Orkaby A. (2022). Frailty and Survival After In-Hospital Cardiopulmonary Resuscitation. J Gen Intern Med, 2022, 37(14), 3554-3561.
- Aggarwal M, Bozkurt B, Panjrath G, Aggarwal B, Ostfeld RJ, Barnard ND, Gaggin H, Freeman AM, Allen K, Madan S, Massera D, Litwin SE, & on behalf of American College of Cardiology’s Nutrition and Lifestyle Committee of the Prevention of Cardiovascular Disease Council. (2018). Journal of the American College of Cardiology, 2018, 72(19), 2391-2405.
- Beezer J, Al Hatrushi M, Husband A, Kurdi A, & Forsyth P. (2022). Polypharmacy definition and prevalence in heart failure: a systematic review. Heart Fail Rev, 2022, 27(2), 465–492.
- Petermann-Rocha F, Lyall DM, Gray SR, Esteban-Cornejo I, Quinn TJ, Ho FK, Pell JP, & Celis-Morales C. (2020). Associations between physical frailty and dementia incidence: a prospective study from UK Biobank. Lancet Healthy Longev, 2020, 1, e58–68.
- Ward DD, Ranson JM, Wallace LMK, Llewellyn DJ, & Rockwood K. (2022). Frailty, lifestyle, genetics, and dementia risk. Journal of Neurology, Neurosurgery & Psychiatry, 2022, 93, 343-350.
- Merchant RA, Morley JE, & Izquierdo M. (2021). EXERCISE, AGING AND FRAILTY: GUIDELINES FOR INCREASING FUNCTION. J Nutr Health Aging, 2021, 25(4), 405-409.
- Theou O, Stathokostas L, Roland KP, Jakobi JM, Patterson C, Vandervoort AA, & Jones GR. (2011). The Effectiveness of Exercise Interventions for the Management of Frailty: A Systematic Review. Journal.
